This article was published in JEMS in 1986, and should be read with an eye for how this topic would have been regarded in that long-ago time.
One of the exciting, but sometimes frustrating aspects of prehospital care is that we cannot choose our "clientele." We have a responsibility to treat all callers with our best efforts, regardless of race, ethnic origin, nationality and religion. But healthcare workers have one additional parameter which can elicit prejudice and the temptation to treat a patient differently: size. Whether a person is obese or unusually long or big, it is the rare helper who can honestly say the patient's size never influences his performance.
Indeed, big bodies are of great concern to field personnel in terms of the logistical challenges posed. People who exceed the average ranges of height or weight can make routine medical care more difficult. Such activities as spinal immobilization, IVs, intubation, and thorough physical examination are sometimes very difficult, if not impossible, to accomplish. And what prehospital worker has not groaned when a call entailed carrying a very large patient down several flights of rickety stairs?
Perhaps by examining the physiologyand common medical consequences of obesity, a more tolerant understanding of patients with big bodies can evolve. Also, it can help to have a few tips in your arsenal of approaches for coping effectively with people who are too tall or too big for prehospital care equipment.

Analysis of Obesity
What is obesity? And who is likely to fall into it? "The average adult living in the U.S. can be expected to gain 15 to 25 pounds between the ages of 25 and 50 years." (1) The weight gain is so gradual that it is hardly noticeable — until a person tries to fit into an old uniform or other clothing from their youth! However, most people do not end up obese in the true sense of the word.
There are many thoughts as to why obesity occurs. These range from learning-theory explanations and psychological issues (unresolved dependency needs, eating for power or to allay depression, to alleviate a sense of inferiority, maladaptive eating behaviors, "addictive" personality) to brain damage, environmental factors, endocrine dysfunction, and hereditary disease. One biopsychosocial model to explain obesity is divided into two schools of thought: 1) a person uses food chronically for non-nutritive purposes; or 2) a person is biologically 'programmed" for fat.
There are probably multiple factors underlying most cases of obesity. The bottom line is that, for some reason, a person has ingested more calories than have been expended by the body and an accumulation of fat stores has occurred; it requires an excess of 3,500 calories to gain a single pound.
The long-recognized standard used by people who focus on obesity for determining ideal body weight is the Metropolitan Life Insurance Company tables. They were originally derived from a Build and Blood Pressure Study done by that company in 1959; the tables were updated in 1983 (see Figure 1).
Obesity begins when a person's body weight is between 20 and 25 percent over the ideals charted on these tables. A person is defined as "morbidly obese" when body weight is 100 percent or more over ideal body weight. Part of the reason the new tables reflect an increase in ideal body weight (particularly among small people) is that in the past decade researchers have found that a certain reservoir of extra weight helps reduce the incidence of cardiovascular disease.
Obesity is a surplus of body fat. Normal ranges of body fat for men are 15 to 20 percent; for women, 20 to 25 percent; and for infants, 14 percent. Thus, obesity is different from the condition known as "overweight," where there is an excess in body weight relative to the standards established for a particular height. While some overweight people are certainly obese, it is not uncommon to find well-muscled people, for example, whose weight doesn't fit the Metropolitan Life tables for their build, yet who are not obese. A prehospital worker with a tired back is probably as unhappy to see a professional football player who will require lifting as an obese person. In fact, the average height of nine of the Chicago Bears football players (not including 'Refrigerator" Perry) is 6'4", while their average weight is 268 pounds. This is well above the ideal weight range of 181-207 pounds allowed for large body frames on the Metropolitan Life table. Even Super Bowlers can be a pain in our sacroiliacs!
Obesity is clearly a problem in the U.S. Fully 30 percent of the population, or about 68 million people, exceed ideal body weight; at least 40 million are obese. Of adolescents, 16 to 20 percent are obese.(2) A study from Framingham, Mass. found that three percent of the males and nine percent of the females were 50 percent or more above their optimum weight. Some sources refer to this as "massive" obesity. The record human weight, as listed in the Guiness Book of World Records, is 1,069 pounds.
It is interesting to note that different socioeconomic groups have varying tendencies toward obesity. Of course, in a society where Twiggy was once the highest paid model, a great deal of focus is placed upon body image. Thus it may not be so surprising to find that obesity is more prevalent among the lower classes, and in groups "not well-acculturated in American society" — in other words, among people who may not so widely subscribe to this aspect of the American dream. (3)
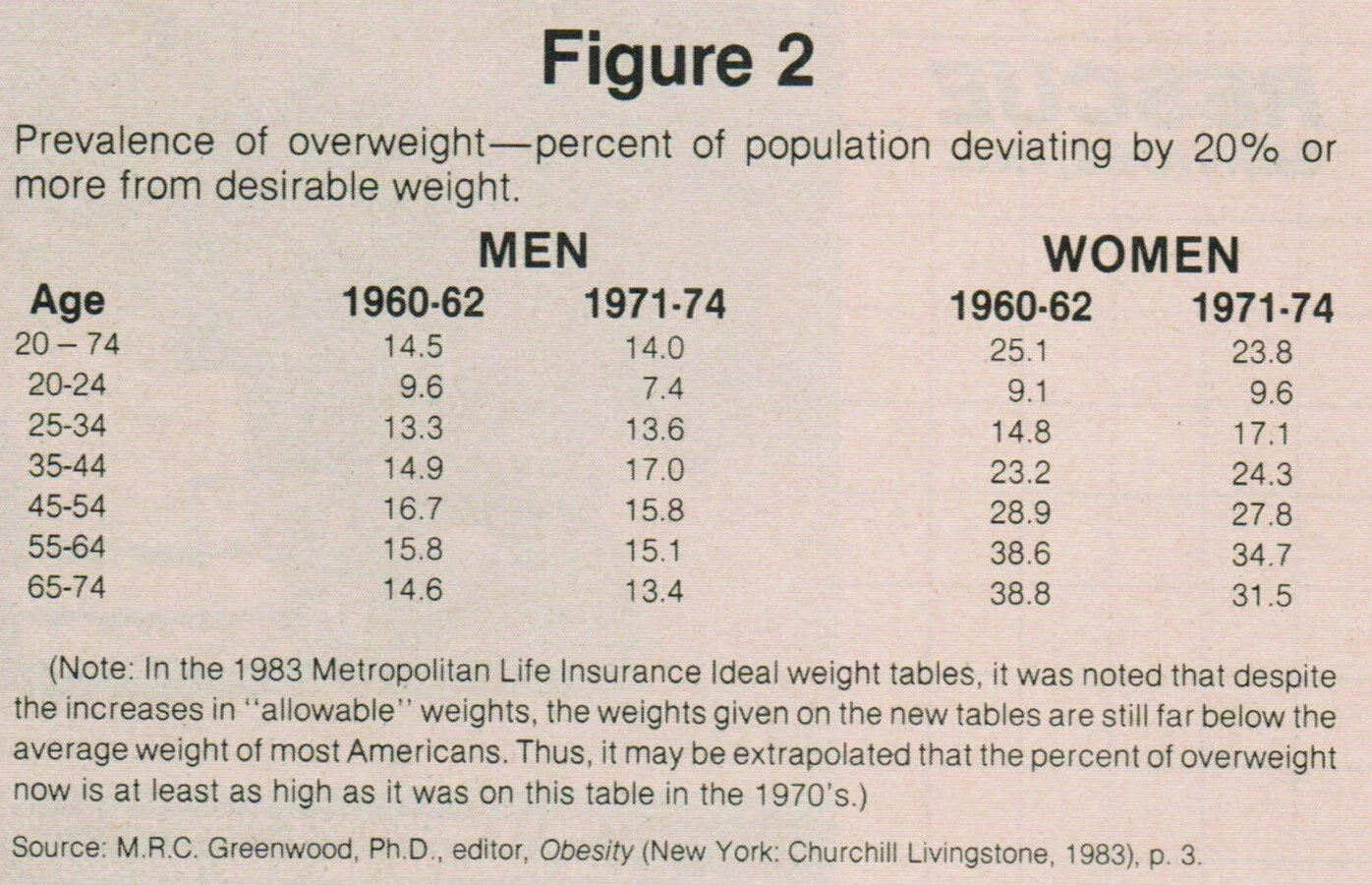
Obesity is more common among women than men. In every age group on the table in Figure 2, the percentage of obese women was significantly higher than the percentage of obese men. Why this occurs has not been determined scientifically, but endocrinology research specialist Trudy J. Yost, RN, of the University of Colorado Health Sciences Center says she sees three kinds of obese women: those who have been "forever chunky," even as infants, those who developed a weight problem at puberty, and those who become obese as an outgrowth of pregnancy.

Rescue personnel need to be physically fit for their jobs in case of the unexpected. Here lifeguards, firefighters, and paramedics struggle with a 300-pound victim during a cliff rescue. Photo by Daren Wannamaker.
The physiology of obesity is an interesting phenomenon. While many people think that all a fat person has to do about a weight problem is try harder to lose it, this prejudice must be placed into perspective if obese people are ever to receive fair tolerance and understanding from their fellow humans. The word obesity derives from Latin for "ob" (over) and "edere," (to eat); this implies a single etiology for the problem, but that perception is inaccurate. Experiments in which people were force fed until they became obese showed that, once back on a regular diet, the majority reassumed their normal body weight naturally.
Indeed, "the formation of fat is an admirable evolutionary development allowing for compact storage of energy reserves, cushioning, insulation, and even esthetic Perhaps it is surprising that appeal abundant fat storage and consequent obesity are not more frequent if one considers the exquisite balance between food ingestion and energy output which must be maintained over many years, during which both activities tend to be somewhat casually controlled."(4)
According to Yost, the obese person originally gets that way — for whatever reason — through the 'hand to mouth" method. The issue of body image is clearly part of the scenario which can lead a person to that first bout of obesity. "The situation is cyclically defeating," said Yost. “If you feel crummy about yourself, you eat, which makes you feel miserable, so you eat some more" which adds layer after layer to the problem.
But then some physiological forces come into play which make the obese person a victim, not of his own inadequacies, but of identifiable processes that can overwhelm whatever good intentions a person has to lose weight. The result is akin to alcoholism, with all the same needs for a shift from societal closed-mindedness and prejudice.
At the cellular lever, each person has a certain number of adipocytes, or fat cells. This number is set by age two, and will not increase, except possibly •in people who become morbidly obese. However, fat cells can uniquely expand, so that their size changes dramatically. 'Adipose tissue mass in an ordinary person is on the order of 10-20 kg. Muscle tissue, the skeleton and the skin are other tissues of comparable mass. The latter tissues can change their total mass to a considerable degree by atrophy or calcium depletion within a range of a factor of approximately 2-3. Adiopose tissue is, however, able to regulate its mass by a factor of about 1,000."(5)
When an adipocyte has been expanded once, according to Yost, it is like a balloon, easier to blow up again. Therefore, once a person has exceeded ideal body weight, the easier it becomes for that person to mushroom in size again. Losing weight is not the biggest problem. However, keeping it off becomes the hard part, thus the unending parade of "miracle" diets that come into vogue constantly. For people with a true weight problem, there is a 90 percent failure rate at keeping weight off once weight loss has been achieved.
What occurs physiologically in obesity, and what triggers the analogy to alcoholism, is that once a person becomes obese, there is a pathological change in the enzyme system that transports fat into the adipocytes. This enzyme, called lipoprotein lipase (LPL), does function in obesity, but, more importantly, functions far more efficiently after weight loss. Thus, LPL in a person with a prior medical history of obesity puts fat into the cells at a more efficient rate than ever. In addition, those adipocytes are forever 'hungry" to be filled again as they once were. Previously obese people, then, face a lifetime of changed eating habits if they want to maintain their weight loss. For example, a 52' woman who has lost 50 pounds and weighs 120 pounds now must eat 15 to 20 percent fewer calories, in order to maintain the weight loss than a woman her size who was never obese.
Medically, obesity can signficantly affect a person's overall well-being. Obese people have increased problems with hips, knees, and ankles, which clearly interferes with the obvious therapy of energy expenditure through exercise; the incidence of arthritis is high. Gallbladder disease, kidney stones, digestive system diseases, and various cardiovascular diseases affect obese people more than the general population. The relationship between obesity and increased atherosclerosis has definitely been shown. Even a 15-20 percent decrease in body weight will favorably affect both hypertriglyceridemia and hypercholesterolemia, according to Yost.

The Pickwickian Syndrome
In morbid obesity, a person may develop 'Pickwickian syndrome," where the sheer weight of body tissue on the chest makes breathing difficult. Colon and rectal cancer in men, and breast, biliary tract and reproductive system cancers in women also have a high incidence in the morbidly obese. It is certainly easy to appreciate that many of the medical complications of obesity are of an emergent nature, and require the skill, sensitivity, and strength of prehospital personnel to provide care and transport of the obese.
Yet the problems of obesity don't stop with a recital of physical complaints. Its psychological effects are both legitimate and real. Unlike many groups of people whose physical and mental disabilities are well-tolerated by people lucky enough to have lives within normal limits, obese people are commonly the subject of derision. They are blamed not only for being ugly or repulsive, but are also accused of being responsible for being that way. Obesity is clearly a social handicap, one which tends to cause much more heartache for the obese person than the physical consequences of the situation.
The relationship of eating habits to obesity is difficult to pinpoint, because so many theories exist. One source cited anxiety, boredom and anger as stimuli for some people to overeat. Many people have noted that the healthcare professions, particularly nursing and prehospital care, seem to include an inordinate number of large people; indeed, our work environment can surely elicit these emotions! And it's far easier, for many people, to sit around the ambulance station snacking on fast food between calls than exercising. In fact, the larger a person becomes, the less and less appealing (and feasible) it is to exercise, creating a negative spiral for good personal health maintenance.
The best therapy for obesity starts with prevention, especially in families where obesity is a problem, since there appears to be a genetic predisposition to it. Up to 80 percent of obese children become obese adults, and their children will often be obese as well. A mixture of both genetic and environmental explanations probably exists for this finding, but it is well-recognized that these people in particular must strive for the maintenance of ideal body weight as a lifelong project. "Obesity could probably be prevented by inculcating more hygienic eating practices in early childhood, but ignorance, indifference, ingrained natural patterns, and commercially vested interests impose formidable barriers."(6)
Other therapies for obesity include acupuncture, removal of adipose tissue, behavior modification, and surgery to make a smaller pouch of the stomach so it can hold less food. None works well. It is the rare person who, once obese, can regain ideal body weight and stay there. “If 'cure' from obesity is defined as reduction to ideal weight and maintenance of that weight for five years, a person is more likely to recover from almost any form of cancer than from obesity."(7)
Perhaps by acknowledging that obesity is not as simple to rectify as it may seem, prehospital workers can carry more empathy into situations involving obese people. It is certainly in our best interests to let a patient's physique interfere as little as possible in the medical decisions to be made and actions to be taken. One source, referring to doctors, spelled out the hazards of doing otherwise; the point can be redirected, obviously, at any health care worker: "... Doctors, as well as others, are prejudiced in terms of fatness. Doctors can be as much the victims of cultural prejudice as the patients whom they victimize. Sometimes the doctor does not know that he is prejudiced. Such a lack of awareness can hurt the doctor's judgment . . . Such a fat patient may lose his individuality and may be abandoned or treated sadistically or vindictively." (8)
Put another way, treating an obese person with any less compassion or appropriateness than you'd like to be treated yourself may pose legal hazards. One lawsuit has been filed by a 400-pound woman who accused an ambulance crew of public humiliation (she claimed they joked that she would give them back-aches) and of dropping her. The company denies the charges. (9)
Pregnancy: Some Associated Issues
One special kind of 'big body"is the pregnant woman. The transient nature of the growth associated with pregnancy is, perhaps, partly why pregnant women cope well with their changed body image.
Weight gain in pregnancy is not all adipose. Total weight gain averages 25-30 pounds, and can be broken down as follows: "fetus, 7-1/2 pounds; placenta and membranes,- 11/2 pounds; amniotic fluid, 2 pounds; uterus, 21/2 pounds; breasts, 3 pounds; and increased blood volume, 2 to 4 pounds. The remaining 4 to 9 pounds is extracellular fluid and fat reserves." The blood volume of a pregnant woman in the third trimester peaks at 30 to 50 percent above pregestational levels. (10)
The development of obesity as a result of pregnancy, according to Trudy J. Yost, RN , of the University of Colorado Health Sciences Center, stems from not returning to prepregnancy weight between pregnancies. A woman who weighs 120 at the beginning of her first pregnancy and begins subsequent pregnancies at higher weights will find the accumulated weight increasingly difficult to lose, risking long-term obesity.
When transporting a pregnant woman who can sit up, it may be more comfortable for her to sit, not on the squad bench (lateral to the direction of motion), but on the bench or captain's chair that places her back to the direction of travel. In quick braking situations, there will be less torque on her abdomen in this seat. Always seatbelt all passengers in the patient compartment, including pregnant people. The chances of serious injury to mother and fetus are greater when safety restraints are not used.
If she must lie down, avoid making her lie flat, as this can be very uncomfortable. The weight of the uterus and its contents can compress the inferior vena cava, interfering with blood flow. Instead, let her lie on her side, if possible, and think to place her in that position if she is unconscious. Even women who must be spinally immobilized can, once strapped to the backboard, have one side of the board raised so that she is effectively lying more on her side than on her back. If possible, she may also prefer to keep her knees bent when lying down.
Dealing With Big Bodies
In the newspaper account of the lawsuit, the ambulance company operations manager was quoted as saying that the women “. . . was so huge that her weight actually overlapped the stretcher. A patient that size is just too big for the ambulance equipment made today." What to do? Equipment is designed for the normal, average human shapes and sizes we usually encounter. In fact, the Ferno-Washington ambulance stretchers are designed to accommodate persons up to 400 pounds. What do you do with a 500-pound person? The longest stretcher mattresses by Ferno-Washington are slightly shorter than 76 inches. What if the patient is longer than 6'4'?
Improvisation often seems like our middle name in EMS. We are asked to go places and accomplish things that many people would consider logistical nightmares. Take, for example, the 807-pound man in his '30s on the second floor who was having trouble breathing. Of course, it was nighttime to boot. The patient was lowered, with considerable planning and mutual aid manpower, out his window, and then lifted by 11 men into the ambulance. A memorable call! (See jems, June 1986, p. 25.)
One thoughtful 600-pounder had her own custom-made wheelchair and provided the six helpers with her own 8 x 10 planks for creating a ramp into the ambulance. Others with morbidly obese patients describe using a fire department tarp as a strong enough material for a blanket lift, with many hands to help. “It's the only way to put handles on a handleless person," said 'Tricks of the Trade' specialist Thom Dick. He also suggests, if the patient is in the bathtub filling the tub with water until the patient floats; that way, a blanket can be worked underneath the patient for extrication. (If it's cold, Thom says, consider replacing it with a dry blanket later. )
Of course, people who weigh more than 300 pounds are seldom encountered, despite one paramedic's experience of transporting three patients in one morning with a combined total body weight of 1,115 pounds! It is far more common to have obese people in a range of 200 to 300 pounds — enough to pose a logistical challenge, yet not enough to make a great "war story." The key is to be honest with your physical abilities at the moment. If you need help lifting, ask for it. If you haven't eaten or slept for 20 hours, don't expect miracles from your body. As always, use good body mechanics in lifting, not your back muscles.
In many cases, bystanders and relatives can be pressed into service. However, inquire whether they have known back trouble; many people will put aside their own safety in order to help, and that's the sort of help you do not need. Communicate clearly what will be done, when, and in what order, so that no one gets hurt.
Use wheels to their best advantage. For example, have the patient lifted and the stretcher wheeled underneath, rather than carrying the patient the few feet to the stretcher. Use stair-chairs, which have wheels, whenever possible. Consider having a roller-board, similar to those used in surgery, installed on the ambulance as an option for dealing with heavy people.
Sometimes the patient is in a place where the stretcher will not fit or where there are turns, such as on a staircase, that make use of the stretcher awkward. Consider using a scoop stretcher or backboard, and snugly strapping the patient onto it, to negotiate difficult terrain until the ambulance cot is accessible. This, like the blanket carry, gives handles to your bulky challenge. However, trying to put a scoop stretcher under a person lying on a bed can be a nightmare; it's easier if the patient is lying on a hard surface.
Finally, recognize that the most likely time to be injured in lifting is during a critical call. If you are out of position, or do not have a good hold on your part of the lifting system, speak up! It may seem that it's all right to take the risk 'just this once," but it only takes a moment to incapacitate yourself. If anything, slow down on critical calls so that extrication is both safe and smooth.
Handling Tall People
Just as our equipment has limitations on bulk, it is limited by patient length. Yet many people over 6'4" require emergency service, and your logistical challenge is made even greater when spinal immobilization is indicated or a traction splint is in use. Generally, a tall person can fit the stretcher by bending the knees; if uncomscious, a pile of blankets can be put under the knees for the same effect. This gives the crew access to the foot-end handle for raising or lowering the stretcher without leaving boot prints on white uniform shirts.
When immobilization is required, consider placing two .backboards under the patient, offset by the needed distance; be sure to secure them together well, or you may end upwith a real problem if they separate. Some paramedics have put very long patients on the stretcher backwards (feet first) so that the overlapping feet could rest on the bench or captain's chair commonly found at the head of the stretcher area. This is especially good for securing the traction splint, when used. Thom Dick even described having to use a pickup truck on one call to transport a person too tall for the ambulance; of course, each case depends on factors such as weather for applying such innovation.
IV Placement
IV placement on obese people can be a significant challenge. However, there are some principles, if applied, that can boost success rates. First, even in cardiac arrest situations, don't hurry! Apply the tourniquet, and then give the veins time to fill. This may require several minutes. Patients who are awake can help by opening and closing the hand to help fill the veins. Be careful about patting or flicking the area with your hand. The veins may become overwhelmed by too much stimulation and fail to stand up well. If the patient can tolerate it, lie him or her flat with the arm dependent, and raise the legs if the patient’s condition allows.
Second, on thinner, healthier patients, practice non-reliance on visual clues; learn to place an IV by feeling veins, not by seeing them. This is a sign of a true IV craftsperson. Teach your fingertips to discriminate subtle changes in textures and resilience of tissue. The structures most similar to veins are tendons; bend the joint involved to determine whether what you are feeling is a tendon.
Some people — particularly those in whom IV placement has always been difficult — can tell you potentially successful sites or particularly bad site choices. Trust them! And don't forget to look on the back side of the forearm, as there is often a more superficial vein there. Some obesity experts use only the antecubital area; remember, this effectively eliminates the more distal options. Others recommend trying to find a hand vein. It depends, of course, on why you're establishing an IV; certain medications, such as D50 or vasopressors, require solid, large veins for safest administration. Capillary fragility is increased in many obese people because they do not exercise regularly.
The important thing to remember when working with people of unusual size is that each one is an individual. True, these people pose peculiar challenges and require innovative problem solving, but there is no reason to act any less compassionately or to limit your wfllihgness to be thorough because of their physique. Yet it happens every day. The medico-legal risks aside, the prehospital worker has a moral obligation not to sit in judgment of any patient because of the common societal prejudices many of us carry into EMS. It seems helpful to know that medical researchers have demonstrated a physiological explanation for obesity that transcends the traditional idea that being fat is an issue completely within the control of the victim. Perhaps someday there will be a cure for obesity — who knows? In the meantime, find a way to enjoy each patient, large or small, so that each will feel less overwhelmed by whatever emergency stimulated the call for your aid.
References
1. Stern, JS: 'Diet & Exercise." Obesity; 69.
2. Daniel, Jr., WA: "Obesity in Adolescence." Psychological Aspects of Obesity: A Handbook; 104.
3. Rodin, J: "Obesity: Why the Losing Battle." Psychological Aspects of Obesity: A Handbook; 32.
4. Ibid; 30.
5. Bjorntorp, P: "The Role of Adipose Tissue in Human Obesity." Obesity, p. 17.
6. Kuo, PT, Conn, HL, and DeFelice, EAds: Health and Obesity, New York: Raven Press, 1983; 16.
7. Brownell, K and Wadder, T: "Behavioral and Self-Help Treatments,Obesity; 40.
8. Allon, N: "The Stigma of Overweight in Everyday Life." Psychological Aspects of Obesity: A Handbook, 158.
9. Flint, Michigan. Journal, June 8, 1986.
10. Olds, SB, London, ML, and Ladewig, PA, ed. , Maternal Newborn Nursing: A Family-Centered Approach, 2nd ed. Reading, Massachusetts: Addison-Wesley Publishing Company, 1984; p. 200.
Bibliography
Bray, GA, ed. Obesity in America. U.S. Department of Health, Education and Welfare, NIH Publication *79-359, November, 1979.
Greenwood, MRC, editor. Obesity. New York: Churchill Livingstone, 1983.
Kuo, P T, Hadley, L, Conn, EA, and DeFelice, EA, ed: Health and Obesity. New Yor$: Raven Press, 1983.
Olds, SB, London, ML, and Ladewig, PA, ed: Maternal Newborn Nursing: A Family-Centered Approach, 2nd ed. Reading, Massachusetts: Addison-Wesley Publishing Company, 1984.
Wolman, BB, editor: Psychological Aspects of Obesity: A Handbook. New York: Van Nostrand Reinhold Company, 1982.